Activity/Rest Activity intolerance (specify level) Activity intolerance, for Disuse syndrome, risk for Diversional activity deficit Fatigue Sleep pattern disturbance Circulation Adative capacity: intracranial, decreased Cardiac output, decreased Dysreflexia Tissue perfusion, altered (specify): cerebral, cardiopulmonary, renal, pastrointestinal, peripheral Ego Integrity Adjustment, impaired Anxiety (mild, moderate, severe, panic) Body image disturbance Coping, defensive Coping, individual, ineffective Decisional conflict Denial, ineffective Energy field disturbance Fear Grieving, anticipatory Grieving, dysfunctional Hopelessness Personal identity disurbance Post-trauma response (specify stage) Powerlessness Rape-trauma syndrome (specify) Rape-trauma syndrome: compound reaction Rape-trauma syndrome: silent reaction Relocaction stress syndrome Self-esteem, chronic low Self-esteem disturbance Self-esteem, situational low Spiritual distress (distress of the human spirit) Spiritual well being, enhanced, potential for | Elimination Bowel incontinence Constipation Constipation, colonic Constipation, perceived Diarrhea Incontinence, functional Incontinence, reflex Incontinence, stress Incontinence, total Incontinence, urge Urinary elimination, altered Urinary retention, (acute/chronic) Food/Fluid Breastfeeding, effective Breastfeeding, ineffective Breastfeeding, interrupted Fluid volume deficit (active loss) Fluid volume deficit (regulatory failure) Fluid volume deficit, risk for Fluid volume excess Infant feeding pattern, ineffective Nutrition: altered, less than body requirements Nutrition: altered, more than body requirements Nutrition: altered, risk for more than body requirements Oral mucous membrane, altered Swallowing, impaired Hygiene Self-care deficit (specify level): feeding, bathing/hygiene, dressing/ grooming, toileting Neurosensory Confusion, aacute Confusion, chronic Infant behavior, disorganized Infant behavior, disorganized, risk for Infant behavior, organized, potential for enhanced Memory, impaired Peripheral neurovascular dysfunction, risk for Sensory perception alterations (specify): visual, auditory, kinesthetic, gustatory, tactile, olfactory Thought processes, altered Unilateral neglect |
| Pain/Discomfort Pain Pain, acute Pain, chronic Respiration Airway clearance, ineffective Aspiration, risk for Breathing pattern, ineffective Gas exchange, impaired Spontaneous ventilation, inability to sustain Ventilatory weaning response, dysfunctional (DVWR) Safety Body tempurature, altered, risk for Environmental interpretation syndrome, impaired Health maintenance, altered Home maintenance management, impaired Hyperthermia Hypothermia Infection, risk for Injury, risk for Perioperative positioning injury, risk for Physical mobility, impaired Poisoning, risk for Protection, altered Self-mutilation, risk for Skin integrity, impaired Skin integrity, impaired, risk for Suffocation, risk for Thermoregulation, ineffective Tissue integrity, impaired Trauma, risk for Violence, (actual)/risk for: directed at self/others | Sexuality(component of ego integrity and social interaction) Sexual dysfunction Sexuality patterns, altered Social Interaction Caregiver role strain Caregiver role strain, risk for Communication, impaired verbal Community coping, enhanced, potential for Community coping, ineffective Family coping, ineffective Family coping, potential for growth Family processes, altered: alcoholism (substance abuse) Family processes, altered Loneliness, risk for Parental role conflict Parent/infant/child attachment, altered, risk for Parenting, altered Parenting, altered, risk for Role performance, altered Socical interaction, impaired Social isolation Teaching/Learning Growth and development, altered Health-seeking behaviors (specify) Knowledge deficit (learning need) (specify) Noncompliance (compliance, altered) (specify) Therapeutic regimen: community, ineffective management Therapeutic regimen: families, ineffective management Therapeutic regimen: individual, effective management Therapeutic regimen: individual, ineffective manageme |
Sunday, April 17, 2011
nursing diagnosis
Physiology and management of normal labour
Labour is more difficult in humans than in most other mammals. Our ancestors, the Australopithecines, adopted the upright posture about five million years ago. Natural selection produced a smaller pelvis, which more efficiently transmits forces from the hind legs to the spine. About 1.5 million years ago brain size began to increase (probably associated with improved social integration and later with the language instinct), with the result that the head of the human fetus at term now takes up most of the available space in the mother's pelvis.

Longitudinal view of fetal head in the pelvis showing how little room there is

Horizontal view of engagement in left occipito-anterior position

Rotation of fetal head as it descends through the pelvis. The maximum diameter of the head matches that of the pelvis at each level (maximum diameters are indicated by an arrow)
It was probably only because of the development of rotation of the head during labour some 300 000 years ago that the system of human birth works at all. The fetal head usually engages in the occipito-transverse position and rotates to occipito-anterior as it passes through the pelvis, allowing the shoulders to engage in the pelvic brim in the transverse position. Once the head is born, the shoulders rotate into the anterior-posterior position, which facilitates their delivery.
The normal uterus is spontaneously contractile, and it is largely the progesterone secreted from the placenta that suppresses activity of the uterus during pregnancy, keeping the fetus within the uterus. In addition, the cervix remains firm and non-compliant. At term, changes occur in the cervix that make it softer, and uterine contractions become more frequent and regular. The precise mechanisms of these changes remain obscure. Changes in the ratio of oestrogen to progesterone, fetal steroid secretion, and changes in the tension of the uterine wall as the fetus grows probably all play a part. Evidence is increasing that the long term interests of the fetus are best served by it being large at birth. However, this represents a problem for the mother, as some women experience long term pelvic damage from delivering large babies. This conflict between the interests of the baby and the mother is probably the reason that the duration of pregnancy is so variable. The mother gives birth more easily if the baby is premature, but the baby survives best if born at term and larger.

Factors implicated in the onset of labour
Stages of labour
Labour can be divided into three stages, which are unequal in length. The fundamental change underlying the process of the first stage is progressive dilatation of the cervix. This gives rise to the familiar symptoms and signs of labour. The cervix is richly supplied with nerve endings, and as it starts to dilate, this gives rise to the characteristic pain of labour. In addition, the plug of viscous mucus that has protected against the ingress of bacteria during pregnancy often emerges as a show. The dilatation of the cervix reduces the support for the fetal amniotic membranes, which bulge through the cervix, and often the rupture of these membranes can be the initiating phenomenon of active labour.
Three stages of labour
- First: from the onset of labour to full dilatation (commonly lasts 8-12 hours in a first labour, 3-8 hours in subsequent labours)
- Second: from full dilatation of the cervix to delivery of the baby (commonly lasts 1-2 hours in a first labour, 0.5-1 hour in subsequent labours)
- Third: from delivery of the baby to the delivery of the placenta (commonly lasts up to an hour if physiological, 5-15 minutes if actively managed)
Under optimal circumstances regular uterine contractions are prompted by the development of contacts between cells considered to be sites of low resistance. These gap junctions are sites of low electrical resistance which allow the passage of depolarisation waves from one muscle cell to another across the uterus. Ideally the process coincides with the ripening of the cervix. If the contractions start or the membranes rupture before the cervix is properly ripe, the process is stimulated by the release of prostaglandins from the membranes and the uterine decidua. Then labour has to pass through a latent phase during which the cervix dilates only very slowly. This can be very demoralising for the mother and increases the risk of infection during labour.

Dilatation of the cervix: (a) cervix not taken up or dilated in late pregnancy; (b) cervix 1 cm dilated; (c) cervix 2-3 cm dilated with a bag of membranes bulging; (d) cervix 5 cm dilated with the membranes ruptured and amniotic fluid escaping
Monitoring labour
Progress in the latent phase of labour is assessed with the Bishop score. The cervix should change at a minimum of one Bishop score point an hour if labour is to end within a reasonable time (only 20% of women move more slowly than this). A score of 11 indicates the onset of the active phase of labour, during which the average rate of cervical dilatation in women in their first labour is 1 cm/h. In parous women the cervix dilates faster—on average 1.6 cm/h.

Latent and active phases of labour in a primiparous woman
An important development in the management of labour was the introduction of the partogram. First developed by Hugh Philpott in 1972 to identify abnormally slow labour, the partogram is a graphical representation of the changes that occur in labour, including cervical dilatation, fetal heart rate, maternal pulse, blood pressure, and temperature; it also shows a numerical record of features such as urine output and the volume and type of intravenous infusions (including oxytocin drips). It is therefore possible at a glance to identify deviations from normal in any of these variables.

Partogram: the broken lines show expected progress of cervical dilatation in multiparous (left) and primiparous (right) women
Bishop score for assessing cervical ripeness
View this table:
It is difficult to predict how a labour will progress; we cannot predict the likely strength and frequency of uterine contractions, the extent to which the cervix will soften and dilate easily, and the extent of moulding of the fetal head. Equally, we cannot know beforehand whether the complex fetal rotation needed for an efficient labour will take place properly. For all these reasons, antenatal pelvimetry has not proved to be a useful predictor, except among those who have had traumatic damage—for example, a fracture of the pelvis.

Essential changes between intrauterine circulation and extrauterine circulation (the bypasses that close at or soon after birth are marked with parallel lines)
Oxygen supply
The oxygen supply is reduced during labour because contractions interfere with the flow of oxygenated maternal blood to the placenta. However, the fetus normally adapts well to this. The fetal circulation is unaffected by contractions (as the fetus is enclosed within the uterus), unless there is cord entanglement with compression. The normal oxygen tension in the fetal blood before labour is about 4 kPa. During labour it falls to about 3 kPa. However, redistribution of the flow within the fetus to protect the vital organs—such as the heart and brain—means that a healthy fetus copes well with this stress.
Delivery of placenta
Once the baby is born, the uterus continues to contract strongly and can now retract, decreasing markedly in size. This shears off the placenta from the uterine wall. If the placenta is allowed to be delivered with normal contractions (sometimes called “physiological management”), this can take up to an hour. Use of an oxytocic drug speeds this process fourfold and reduces average blood loss by about 50%. A recent study published in the Lancet showed that in a large randomised controlled trial only 6.8% of women receiving active (drug) management had significant bleeding, compared with 16.5% receiving physiological management.

Meta-analysis of effects of prophylactic oxytocic drugs in blood loss during third stage of labour
Use of drugs
Oxytocic drugs should be given with the birth of the anterior shoulder. The use of antenatal ultrasound screening has virtually eliminated the possibility of giving the oxytocic before the birth of an undiagnosed second twin. Syntocinon is the most used oxytocic known to be effective; the addition of ergometrine may reduce blood loss even further but can cause serious hypertension in susceptible women—for example, those with pre-eclampsia. Because of the speed with which the uterus retracts after stimulation with an oxytocic, the placenta should be removed by controlled cord traction as soon as it is perceived to have separated from the uterine wall.
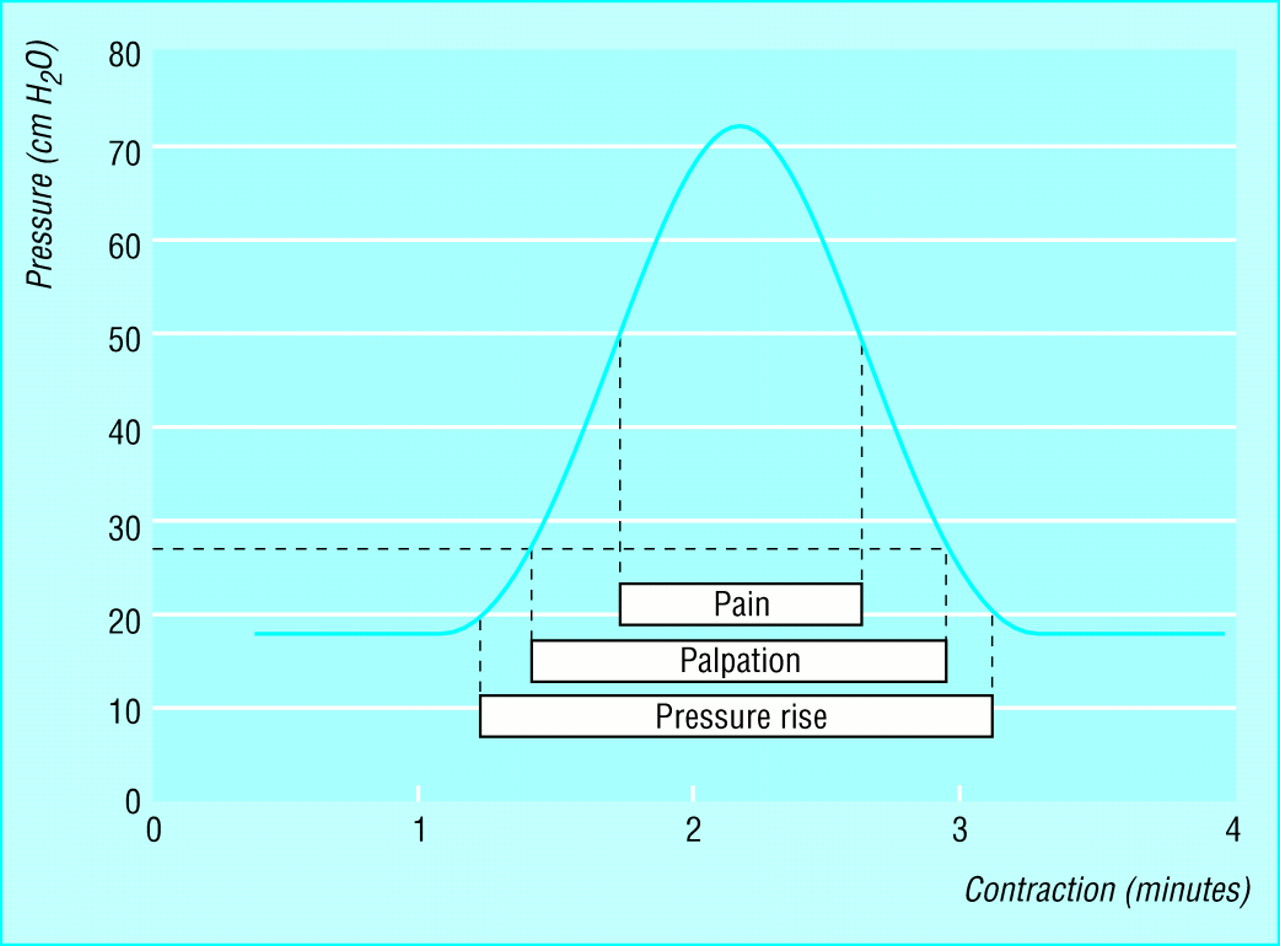
Pressure recording of a uterine contraction in the later first stage of labour (note differentials of pressure rise with objective palpation of contractions and pain felt by the mother)
Support for mother
As most labours are spontaneous and end with a normal delivery, the main purpose of the birth attendant (usually a midwife) is to provide support for the mother and her partner in labour and to monitor the process for abnormality. The birth attendant therefore needs to understand both the physical processes and the emotional needs of the mother.
It is difficult for a nulliparous woman to understand the sensations (including sometimes severe pain) that she will experience during childbirth until they actually occur. The birth attendant therefore needs to interpret the woman's sensations for her—for example, explaining that fears that “the baby is stuck” and “my perineum is going to split apart” are normal and do not necessarily indicate an abnormality.
Some women need a quietly supportive approach; others need boisterous encouragement (especially while pushing in the second stage). Sensitivity and experience are needed to match the type of support with the needs of the mother.

Delivery in a standing position
Delivery positions
Because women in labour are in pain they often feel the need to move around a great deal. It is therefore helpful to provide an environment in which the woman can vary her position at will—for example, soft mats and bean bags on the floor, cushions, or birth pools. The woman should be encouraged to deliver in whichever position she feels comfortable, providing that this does not affect the fetus significantly. Some women like standing or squatting, but the most commonly used position is lying propped up on a bed; the only position that should routinely be proscribed is the supine position (that is, with the woman flat on her back). This often causes caval compression, restricting venous return from the legs, and can result in the supine hypotension syndrome, leading to fetal and maternal hypoxia. If the supine position has to be used—for example, for vacuum or forceps delivery—a wedge should be placed under the mother's buttocks and lower back to tilt the uterus away from the inferior vena cava.

Delivery in hands and knees position
Other roles of birth attendant
The value of physical guidance of the fetus by the attendant at a normal birth is controversial. The HOOP (“hands on or poised”) study, in which control of the emergence of the head and shoulders is being compared with entirely spontaneous birth is still under way.
After the birth, the birth attendant should be vigilant for any signs of haemorrhage or infection.
placenta and umbilical cord
Placenta and Umbilical Cord
The placenta may be usefully understood as a "parasite" feeding on blood from the endometrium. Imagine scooping out a portion of the endometrium. The resulting bowl will fill with blood from broken vessels in the endometrial stroma. Now lay a cover over the bowl, and imagine many "roots" extending down from the cover into the blood-filled hollow. The roots can can absorb oxygen and nutrients from the blood in which they are bathed.
The cover is the chorionic plate of the placenta. The "roots" are the chorionic villi.Both the placenta and the chorionic villi are entirely fetal tissue (orange in the diagram above). "Anchoring villi" attach the placenta to the endometrium. Smaller branching villi extend out into the intervillous space. Fetal circulation passes down the umbilical cord, though vessels in the villi, and back up the umbilical cord.
Maternal blood "spills" from open endometrial arteries (the spiral arteries) into the intervillous space (pink in the diagram above), and returns into endometrial veins. Thus the chorionic villi are surrounded and bathed by "lakes" of maternal blood. Within the intervillous space, maternal blood is not contained by blood vessels.
The surface of the chorionic villi is an epithelial layer, the fetal syncytiotrophoblast, which has the ability to grow invasively into the maternal endometrium. The syncytiotrophoblast also has microvilli on the surface for absorbing nutrients from maternal blood.
In the extravagant name "syncytiotrophoblast", syncytio- tells us that this is a syncytium, a tissue in which many nuclei occupy a large cytoplasmic volume without separation into individual cells (skeletal muscle fibers are a more familar example of syncytial tissue); tropho- tells us that this tissue provides nutrition; and -blast tells us that it is growing.Forming the core of each chorionic villus is mesenchymal stroma containing fetal blood vessels.
Beneath the syncytiotrophoblast (i.e., toward the core of the villus), is the cytotrophoblast, a layer of cuboidal cells which eventually disappear. (The cytotrophoblast also forms trophoblast columns, masses of cells filling the ends of anchoring villi.) Maternal endometrial stromal tissue adjacent to the placenta differentiates into large decidual cells (so named because the outer layer of the endometrium is shed at birth along with the placenta). Decidual cells may intermix with fetal cells in the cytotrophoblast. The boundary between maternal and fetal tissue is immunologically interesting.
For micrographs of placenta, see WebPath (decidual cells), WebPath (first trimester chorionic villi), WebPath (second trimester chorionic villi), and WebPath (third trimester chorionic villi).
Between maternal blood and fetal blood lies the thin syncytiotrophoblast and the fetal capillary endothelium, across which all exchange of gases, nutrients, hormones, and wastes occurs.
- Fetal circulation is entirely closed, confined to vessels within the chorionic villi.
- Maternal blood flow though the placenta is open. "Lakes" of maternal blood fill the intervillous space, uncontained by any endothelial lining.
The umbilical cord is simply a conduit carrying fetal blood between the fetus and the placenta. It normally contains two arteries and one vein, surrounded by extensive mesenchymal tissue ("Wharton's jelly").
 |  | | |
Wednesday, April 13, 2011
NCLEX Review and Secrets: NCLEX Review about Cardiac Nursing (46-50)
Cardiac Nursing
about Cardiac Nursing 46. The nurse is caring for a client with congestive heart failure. On assessment, the nurse notes tha..."
about Cardiac Nursing 46. The nurse is caring for a client with congestive heart failure. On assessment, the nurse notes tha..."
Subscribe to:
Comments (Atom)